
Electrophysiologists Manuel Ayala Patete, Dulce Garcia, Mikel Liñero, Vanesa Burgos and Carlos Garcia Lithgow, all from Centro Cardio-Neuro-Oftalmologico y Transplante (CECANOT) in Santo Domingo, Dominican Republic, write about their experience using the ColumbusTM 3D EP Navigation System (MicroPort) at their institution.
In recent years, three dimensional (3D) mapping for ablation of complex arrhythmias has become routine and necessary in electrophysiology (EP) laboratories. A standard laboratory for treatment of arrhythmias should include a cardiac 3D mapping system to facilitate complex procedures such as ablation of atrial fibrillation (AF) and ventricular arrhythmias. CARTO (Biosense Webster) and EnSite Velocity (St Jude Medical) are the commonly used systems worldwide.
However, according to the latest Latin American Report of Arrhythmias (Keegan et al, Europace 2015;17,794–800), only 42% of the arrhythmia laboratories in the Latin American region have a 3D mapping system and only four laboratories have two systems.
Over the past two years, we have been working at our centre in the Dominican Republic with the ColumbusTM 3D EP Navigation System. This technology is based on electromagnetic tracking of the irrigated ablation catheter FireMagicTM 3D and a single patch placed on the patient’s back with an electromagnetic field generator under the operating table.
The ColumbusTM 3D EP Navigation System has helped to improve the life of local patients suffering from complex arrhythmias—to a large extent—and has allowed physicians to treat complex arrhythmias with satisfactory results. The system is user-friendly and includes a new ECG recording module. From August 2014 to August 2016, 222 cases of patients between seven and 90 years-old (55% female) were performed using the ColumbusTM System.

The most frequently treated arrhythmia was ventricular arrhythmia without structural heart disease (35%), followed by atrioventricular nodal re-entrant tachycardia (AVNRT) (22%). Fifteen per cent of AF patients underwent pulmonary vein isolation.
The immediate success rate was 87.5% for ventricular arrhythmia and 98% for AVNRT. Pulmonary vein isolation in AF was achieved during the procedure in 95% of cases. The complication rate in all procedures was 1.1%, most commonly vascular (72% of all complications).
The ColumbusTM System has proved to be reliable for treatment of the simplest to the most complex arrhythmias, in various age groups, with comparable results to other 3D mapping systems. The complication rate is also comparable to that described in other records.
In our centre, the ColumbusTM System helped to launch our ablation programme thanks to its accessibility and the possibility that a single machine can have a 3D mapping system and an ECG recording module integrated.
During this period, we have performed significant cases such as an incessant AVNRT in a 32-week pregnant woman, an ischaemic storm in a 57-year-old male and ablation of an unsustained ventricular tachycardia in a seven-year-old child.
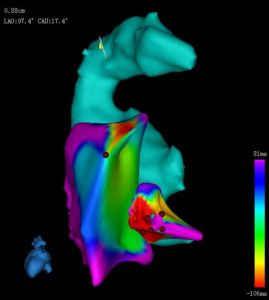
We have also seen the evolution of the ColumbusTM System, from having only the ability to make maps point-by-point to the currently developed real-time mapping (RTM) function. That is a true evolution that allows faster mapping and a more suitable anatomy. (Figure 1).

Another advantage of the ColumbusTM System is real time display of the FireMagicTM 3D catheter curve because multiple magnetic sensors are embedded. The system also allows reviewing of previous catheter curve, catheter position and mapping information of the interesting point when this is selected again.
Another benefit we have achieved with the ColumbusTM System is bringing 3D technology to the treatment of arrhythmias such as atrioventricular reciprocal tachycardia (AVRT), AVNRT, typical atrial flutter, etc, which were not previously accessible due to high costs. This achievement improves efficiency and reduces fluoroscopy time in these procedures.
In our opinion, the ColumbusTM System is ideal when you start a programme of radiofrequency ablation of all arrhythmia substrates or to complement a programme with another 3D mapping system. It is striking that you can make a lot of cases of most arrhythmia substrates at a reasonable cost and in this way “massify” invasive treatment of arrhythmias.
In conclusion, the ColumbusTM System has been successfully placed in our laboratory, and has helped us to be comparable to large laboratories in the region in terms of statistics and number of complex cases solved.
Manuel Ayala Patete is head of Arrhythmias at Centro Cardio-Neuro-Oftalmologico y Transplante (CECANOT) in Santo Domingo, Dominican Republic; Dulce Garcia and Mikel Liñero are associates, Vanesa Burgos is intern in Arrhythmia and Carlos Garcia Lithgow is chief of Hemodinamic laboratory at the same institution.











