
This article has been sponsored by Abbott
Case description
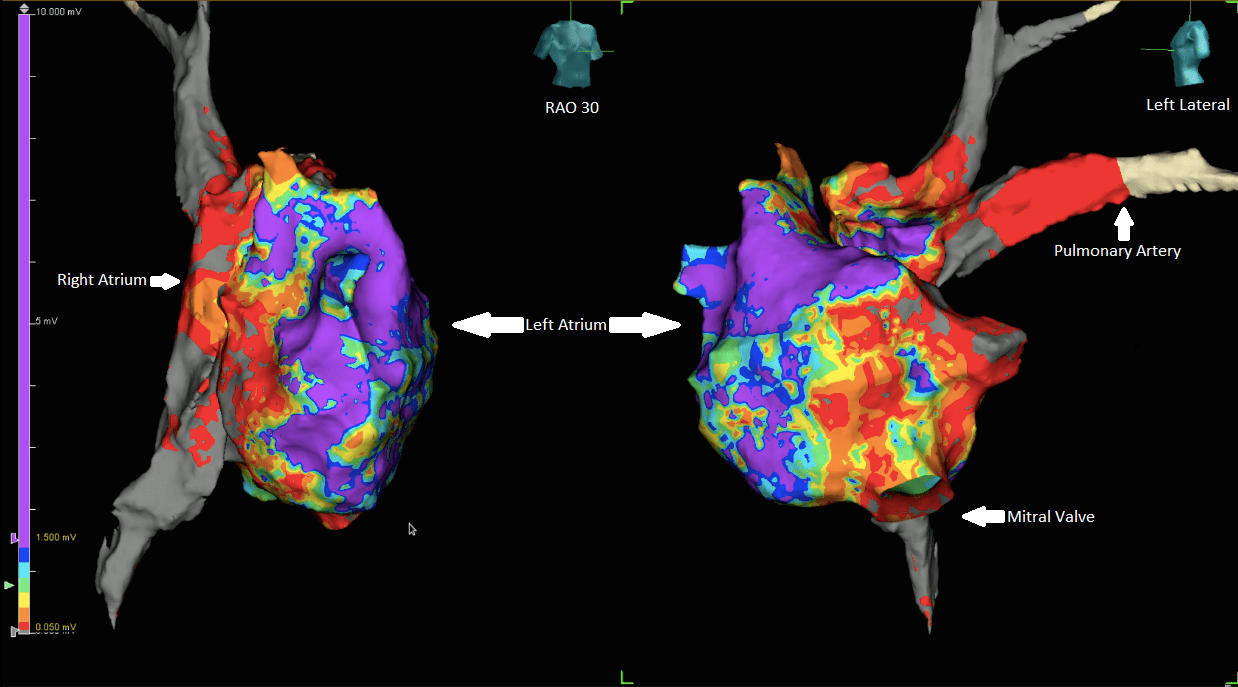
A 31 year-old female with tricuspid atresia and normally related great vessels who underwent an atriopulmonary Fontan (total cavopulmonary anastomosis) at two years of age and a subsequent Fontan revision to a fenestrated lateral tunnel Fontan with a biatrial cut-and-sew modified Cox-Maze operation (both left and right atrial lines) at the age of 11, presented with recurrent intra-atrial reentrant tachycardia refractory to dofetilide and anti-tachycardia atrial pacemaker therapy. She was taken to the electrophysiology lab to attempt an ablation due to the refractory nature of her tachycardia and symptoms related to the tachycardia. The tachycardia was induced and then mapped using the Abbott Ensite Precision Cardiac Mapping System™. With the use of an Agilis™ sheath and the Advisor HD Grid™ catheter, we created a high density voltage and timing map both inside the lateral Fontan circuit (referred to as the right atrium) and in the left atrium through the Fontan fenestration. The map was created using the novel HD Wave Grid map which reduced overestimating areas low voltage by taking the highest overall voltage across the Grid electrode pairs.
The map included 197,352 points taken with the Advisor HD Grid™ and FlexAbility SE™ catheters. Signals were measured within a window of interest spanning 98% of the tachycardia cycle length. Surface score matching was used to eliminate inclusion of far-field ventricular signals. Cycle length stability filtering was set to +/-10ms. The absolute peak of the bipolar signal within the window of interest was used for timing annotation, which allowed for rapid identification of near-field activation in zones with conduction block and wave front collision, and no manual annotation was required. In addition, fewer than 50 points required editing. These points were used for voltage and timing assessment.
We identified multiple lines of conduction block, numerous areas of slow conduction, and several bystander wave fronts that encompassed the entire cycle length of the tachycardia in both the right and the left atria. A wave front utilising a narrow corridor in the mitral isthmus was ultimately identified and ablated, resulting in clean termination of the tachycardia and non-inducibility of any further tachycardia.

Summary
This case highlights the ability and utility of the Advisor HD Grid™ catheter and mapping system to rapidly map atrial arrhythmias in complex congenital heart disease following prior surgical ablation. The ability to rapidly map multiple chambers of the heart with high fidelity may increase the success rate of ablations in patients with challenging anatomy due to congenital heart disease.
Rx Only
Brief summary: Prior to using these devices, please review the Instructions for Use for a complete listing of indications, contraindications, warnings, precautions, potential adverse events and directions for use.
By Philip L Wackel and Bryan Cannon, both paediatric cardiologists from the Mayo Clinic, Rochester, USA








