
The link between cardiac diseases and stroke is well known and reported. Wolfram Döhner writes in Cardiac Rhythm News about the needs for interdisciplinary thinking and collaboration.

Stroke is a leading cause of death and the main cause of physical disability, dementia (second to Alzheimers disease), depression and falls. Up to about one third of patients die within the first weeks after stroke but 60% of patients live with at least minor handicap and about 25% of patients with severe disability and substantial disruption of their previous life. Thus stroke is a major burden to patients and families as much as to the health care systems and the society. Despite improving therapies and decreasing mortality rates in recent years, hospitalisation numbers are increasing. Therefore, long-term care and secondary prevention of stroke will be of increasing importance in respond to the increasing prevalence.
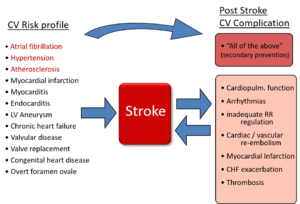
The strong interaction between cardiac diseases and cerebrovascular incidents is well established. About 25% of the ischaemic stroke are of cardioembolic origin and a further 20–25% are of suspected cardiac origin or involvement. Virtually any cardiac pathology (structural, functional, rhythmogenic) may account for an increased risk of stroke. Accordingly, stroke patients frequently have pre-existing cardiac/cardiovascular diseases, that may or may not be diagnosed at the incident of a stroke. But this is not the only and not the foremost reason why a close cooperation of cardiologists with neurologists in comprehensive stroke care is of high and increasing relevance (figure 1).
Cardiologic expertise is needed in stroke care
In the acute, subacute and chronic phase after stroke there are multiple complications and sequelae of stroke that require the involvement of cardiologic expertise. Monitoring and immediate response to stroke induced complications is the main purpose of the stroke unit treatment that is a corner stone in modern stroke therapy and that substantially contributes to improved outcome.
Many of these complications relate to cardiac function, rhythm control or pre-existent cardiac diseases. The most common cardiac complication in the acute phase after stroke include arrhythmias (both, atrial fibrillation and ventricular arrhythmias), temporary breakdown of blood pressure regulation, myocardial damage and elevated troponin levels, or acute complications of pre-existing cardiac pathologies such as infective endocarditis, myocardial infarction or exacerbated heart failure. Previous studies have shown that presence of cardiac complications account for increases in mortality compared to patients without them. While the detection of atrial fibrillation is predominantly pursued to clarify the potential cardio-embolic origin of the stroke, the rhythm monitoring at stroke units is also required to observe potentially life threatening ventricular arrhythmias.
Another complication is the stroke induced myocardial injury identified by increased troponin levels than can be observed in up to 60% of patients when using high sensitivity assays. Of course not all of these patients require immediate (invasive) cardiovascular diagnostic workup, but the number of patients with a culprit coronary lesion has been reported to be 24%. It therefore requires consequent and qualified cardiologic involvement to decide the further diagnostic and therapeutic path of these patients. The pathophysiologic mechanisms of stroke triggering myocardial damage are not completely understood but neuronal signals may be similar to those of the Tako Tsubo Syndrome, only with somatic brain injury. Notably, particularly involvement of the right insular cortex is often seen in strokes with accompanying by myocardial injury. Monitoring dynamic changes in troponin levels rather than singly time measurement and the combination of biomarker assessment with clinical symptoms, ECG and further information such as risk profile and case history may be required to come to a conclusive picture about the need for further cardiac workup.
Beside neuroendocrine activation after stroke also inflammatory immune response may trigger multiple pathways resulting together in a range of cardiac complications including plaque instability, calcium overload, blood pressure peaks, endothelium dysfunction, microcirculatory failure, and electrical instability (Figure 2).
A key diagnostic tool to evaluate cardiac comorbidity is of course echocardiography. Depending on the clinical question to be addressed the decision on the appropriate method (transthoracic or transesophageal echocardiography) may as well have practical implications on patient handling and resources. In a case of suspected infective endocarditis the stroke—that accounted for hospital admission and that is the most overt clinical problem of the patient— represents only one minor criteria of the Duke criteria and further efforts with particular emphasis on cardiac imaging are required to establish the true underlying disease. Again, a close cooperation between strokeologists and cardiologists is required to coordinate these appropriated diagnostic measures.

The stroke patient is a chronic patient who needs continued specialised medical treatment
After the acute phase of stroke continued efforts are required to establish previously undetected cardiac diseases and to target risk factors with consequent and long term strategies of secondary prevention. Cardiologist ‘s collaboration in the long term care of patients after stroke is urgently required as complications are particularly prevalent in patients with stroke
ESC Council on stroke
The European Society of Cardiology (ESC) aimed to improve awareness of stroke among cardiologists in Europe and to promote clinical education and scientific efforts towards stroke. On that basis, the ESC Council on stroke was founded in 2016 and an extensive agenda of activities has been implemented by the council including joint sessions with partner societies, position papers, webinars and cardiovascular round tables. A major activity is the annual international “ESC Heart & Stroke” conference of the ESC Council on stroke that has been established as a clinical educational meeting. All ESC members with interest in stroke are encouraged to get involved to contribute to the stroke council activities.
More work is needed to improve collaboration and integrated treatments concepts in the field of stroke bringing together all specialties involved in comprehensive modern stroke care.
Wolfram Döhner, Stroke Research Berlin and Department of Cardiology, DZHK (German Centre for Cardiovascular Research), partner site Berlin, Charité Universitätsmedizin Berlin, Germany








Thank, Prof Wolfram Döhner. We met in recent ESC Heart and Brian workshop in Prague. This is very interesting and important article as we have also discussed about Stroke in “Heart and Brain Workshop.” It is actually important that we need collaboration and integrated treatments concepts in the field of stroke by multidisciplinary teams between Cardiology and Neurology.
Thank, Prof Wolfram Döhner.