

Cardiac imaging has emerged as an integral part of mapping and ablation in a variety of complex arrhythmias. Advances in imaging techniques, especially the multimodalities technique, have made it possible to map and ablate the more difficult and complex ventricular tachycardias (VT) such as VTs with multiple morphologies, multiple foci and mechanisms, and more recently, VTs of epicardial origin and those with complex congenital heart diseases; Mohammad Shenasa (San Jose, USA) writes for Cardiac Rhythm News.
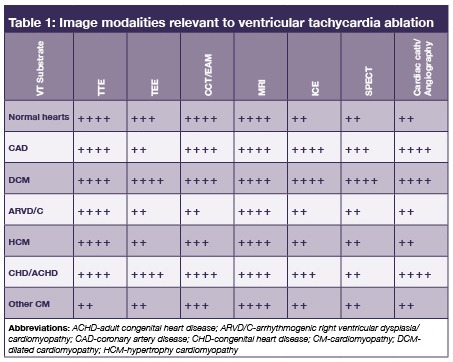
Imaging is generally done before (pre-procedure), during (peri-procedure), and after (post-procedure). The value of each imaging modality varies according to the type of arrhythmia, patient’s anatomy, structural and functional substrate, etc (see Table 1).
Cardiac mapping and imaging is at its unprecedented stage from molecular, multi-modality, and non-invasive imaging as well as real-time scanning and yet is far from perfect. Real-time scanning and compatibility with other modalities is currently under investigation and should arrive to the practice shortly.1 Table 2 demonstrates many possibilities of imaging integration of different modalities. The ideal mapping/imaging technique should therefore be accurate with high specificity and sensitivity, user friendly, capable of matching anatomy with physiology (function) as well as demonstrate the electrophysiological and structural substrate in specific patients, pathology, and arrhythmia.

Electroanatomical mapping (EAM) has been in routine practice for more than two decades and is capable of merging with other technologies such as echocardiography (transthoracic (TTE) and transesophageal (TEE)). Recently, intracardiac echocardiography (ICE) has been used more often and can be merged with EAM (CARTOMERGE Image integration module). Cardiac computerised tomography (CT) and cardiac magnetic resonance imaging (MRI) are now an integral part of today’s cardiac mapping and ablation procedures, and are used for both the diagnosis and evaluation of therapeutic modalities of complex arrhythmias.
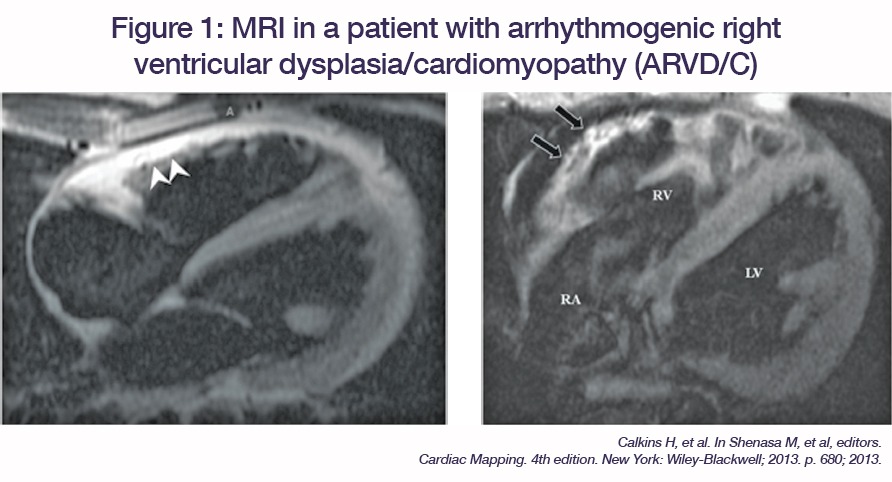
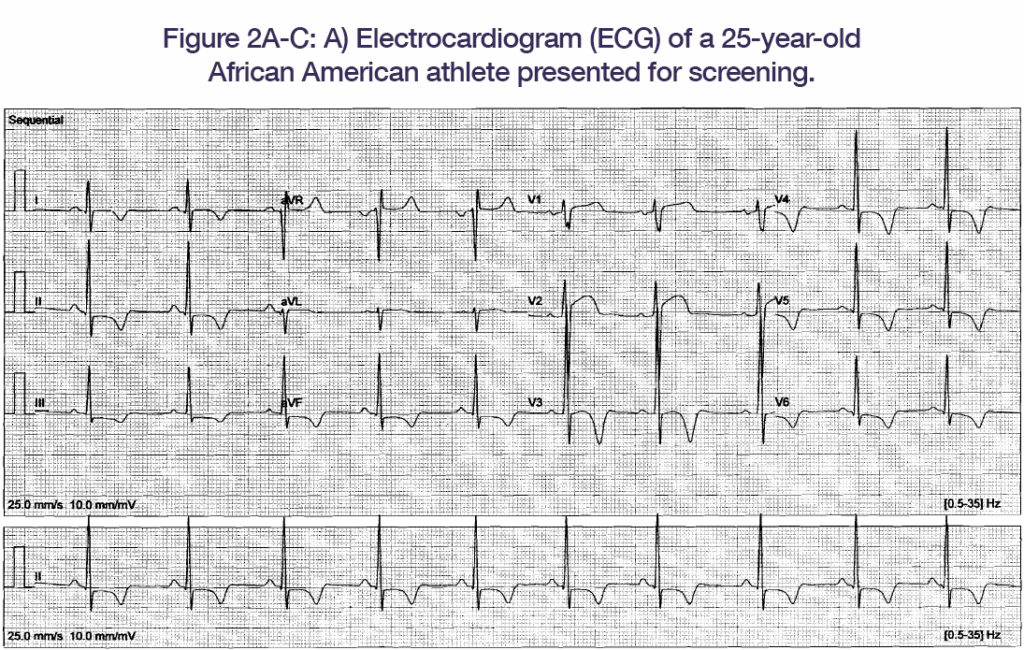
The basics of T1 mapping has been discussed in detail elsewhere and does not need to be repeated here.2 Indeed, this imaging modality is useful in certain substrates such as arrhythmogenic right ventricular dysplasia/cardiomyopathy (Figure 1), hypertrophic cardiomyopathy (Figure 2), dilated cardiomyopathy, and others where simultaneous endocardial and epicardial evaluation of arrhythmogenic substrate is necessary.
 An advantage of cardiac MRI as compared to cardiac CT includes zero ionising radiation (radiation-free). The new generation of cardiac MRI systems and their software workstation should be capable of 3D imaging, which includes the cardiac motion, volume, mass, etc. Furthermore, the new systems reduce the image time significantly. Currently, the use of cardiac MRI suites that allow electrophysiology and ablation procedures are under investigation.3 The wish list for the electrophysiologist includes a more user friendly and cost effective system that is capable to merge and communicate with other systems (i.e. multi-modality).
An advantage of cardiac MRI as compared to cardiac CT includes zero ionising radiation (radiation-free). The new generation of cardiac MRI systems and their software workstation should be capable of 3D imaging, which includes the cardiac motion, volume, mass, etc. Furthermore, the new systems reduce the image time significantly. Currently, the use of cardiac MRI suites that allow electrophysiology and ablation procedures are under investigation.3 The wish list for the electrophysiologist includes a more user friendly and cost effective system that is capable to merge and communicate with other systems (i.e. multi-modality).
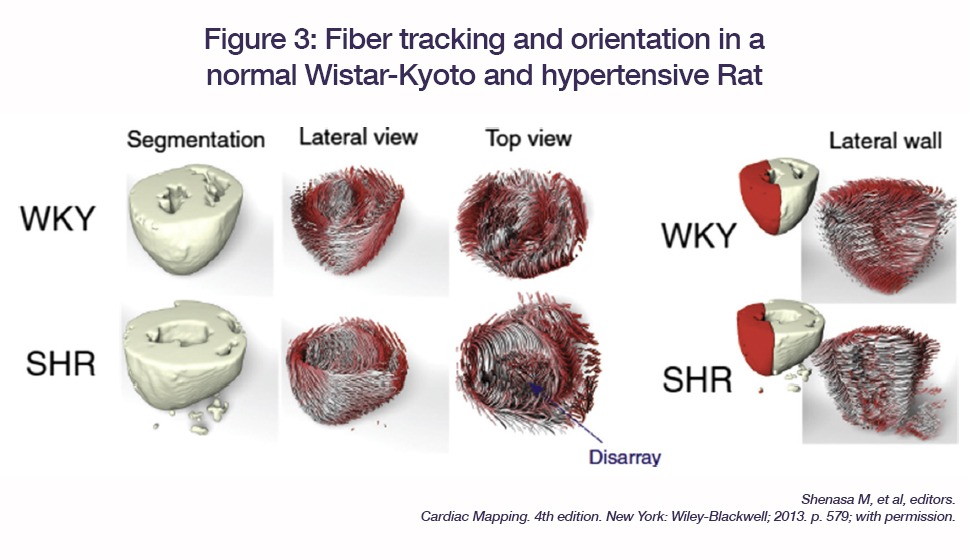
Importantly, new software and sequences allow fibre tracking and orientation to evaluate early detection of cardiomyopathies, progression of the disease, and differential diagnosis such as left ventricular hypertrophy in hypertension, athletes, and hypertrophic cardiomyopathy (Figure 3).4‒6
Summary and future directions
Cardiac imaging relevant to VT should be customised, i.e. patient-specific according to the type of VT, substrate, planned procedures, etc. In the near future, the novel cardiac MRI contrast agents will allow tissue-specific targets for a specific pathology and arrhythmia type. Further studies and randomised trials are warranted to compare head-to-head diagnostic yield with other systems.7 Other emerging imaging modalities include ECG-I (electrocardiographic imaging), myocardial elastography, electromechanical wave imaging, and molecular MRI are on the horizon.
Cardiac MRI has emerged as a routine in today’s management of cardiac arrhythmias including lesion assessment, comprehensive assessment of cardiac morphology and function and tissue structure.8 In simple words, it is a non-invasive biopsy in certain pathologies such as cardiac sarcoidosis, amyloidosis, pericarditis, and other infiltrative pathologies. Most importantly, the imaging modalities should be capable to evaluate the magnitude of fibrosis and lesion formation during ablation and detect patients at a risk of recurrence. Figure 4 shows the future interventional electrophysiology suite where all of the imaging modalities are in a real-time fashion.

References
- Shenasa M et al, The future of cardiac mapping: Dawn of a New Decade, in Cardiac Mapping, M Shenasa, Editor. 2013
- Taylor AJ et al. JACC Cardiovasc Imaging 2016;9(1):67‒81
- Hilbert S et al. Real-time magnetic resonance-guided ablation of typical right atrial flutter using a combination of active catheter tracking and passive catheter visualization in man: Initial results from a consecutive patient series. Europace 2015
- de Marvao A et al. JACC Cardiovasc Imaging 2015;8(11):1260‒9
- Ho CM et al. N Engl J Med 2010;363:552‒63
- Coelho-Filho OR et al. Circulation 2013;128(11):1225‒33
- Wijnmaalen AP et al. Eur Heart J 2011;32(1):104‒14
- Ilg K et al. JACC Cardiovasc Imaging 2010;3(3):278‒85
Mohammad Shenasa is with the Heart & Rhythm Medical Group in San Jose, USA










